
Developing a New Medicine or Device
secondscount.org
There are five basic stages of development that a novel treatment must pass through before approval. Many good ideas for novel treatments don't even make it through these stages due to a variety of factors such as incomplete paperwork or lack of funding. A collaboration involving researchers, doctors, regulators and the private company that owns the patent on the medication or device determine how the trials are set up. Although clinical trials for device approval typically require enrolling fewer patients than do drug trials, this gap has been narrowing as device trials are subject to increasingly rigorous scientific standards.
The Five Stages of Development
The five key stages of clinical trials that a novel device or medication must pass through before - and after - it reaches the market include:

Preclinical
The safety and effectiveness of experimental medications or devices are evaluated in test tubes, computer models and often on animals. For medicines, this involves assessing how the compounds move through living organisms and what impact they have against the disease target. Likewise, devices also must be evaluated for how compatible they are with the human body and how they work within the body.
The main goal of preclinical studies is to rigorously assess safety before human tests begin; this is why preclinical studies often take three to six years (or longer) to conduct. Some preclinical safety tests continue even after the start of clinical trials to help identify any long-term adverse effects. Once ready for the next stage of testing on humans, the researcher or scientist must file an investigational medicine or device application with the U.S. Food and Drug Administration (FDA) before human testing may begin. The application must show:
Results of preclinical experiments
The chemical structure of the compound or design of the device
How it is thought to work in the body
Any side effects found in animal studies; and
How it will be manufactured.
The application must also include a detailed plan of how, where, and by whom the clinical trial will be conducted.
In addition, all clinical trials must be approved and monitored by an Institutional Review Board (IRB), a committee that reviews biomedical and behavioral research involving humans. An IRB is typically set up by academic institutions and medical facilities, but they can also be created by for-profit companies and are called independent or commercial IRBs. The aim of the IRB is to protect the rights and welfare of those involved in the study. Progress reports on clinical trials must be submitted at least annually to IRBs and the FDA.
Pilot, or Phase 1
Researchers first test an experimental medication or device in a small group of people to evaluate its safety, determine a safe dosage range and identify side effects. To establish the safety profile of an experimental medication and determine how it moves through the body, a pilot study may involve 20 to 100 healthy volunteers. Somewhat fewer participants (a dozen or more) are needed for devices. This process can take from six months to a year to complete.
Feasibility, or Phase 2
The experimental medication or device is given to a larger group of patients who have the disease or condition to test whether it is effective and further evaluate its safety. For medications, these trials can involve 100 to 500 participants. Typically the group is divided in two, with one half given a placebo (an inactive substance, often called a "sugar pill"), and the other given the "active" medication. The placebo group is referred to as the control group.
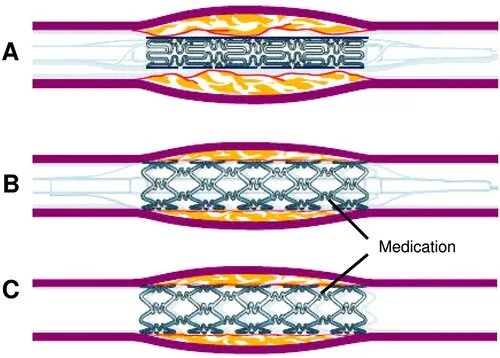
In device trials, rather than implant an inactive device, the control group typically receives the standard treatment for the disease or condition. The goal of this phase is to prove whether the therapy effectively treats the disease. Researchers continue to evaluate the safety of the medication or device, look for side effects and adjust the therapy (such as dosage level). These studies also typically take from six months to a year.
Pivotal, or Phase 3
The pivotal stage is the phase of clinical trials designed to evaluate safety and effectiveness (efficacy) on a wide sampling of participants - from hundreds to 5,000 or more - of the target patient group. For medications, these are large, randomized (that is, the participants are randomly assigned to one of two or more treatment "arms," or groups), placebo-controlled trials that generate statistically significant data. This means the results are unlikely to have been reached by chance or coincidence.
Researchers closely and regularly monitor patients to confirm effectiveness and identify adverse events or side effects. They compare the safety and effectiveness of the new therapy to treatments already in common use for the targeted disease or condition. These studies can take from one to four years to complete, depending on the design of the study and how long it takes to recruit enough patients to meet the minimum size requirements established for the trial.
After Phase 3
Once the three phases of the clinical trials are complete, the data are analyzed to determine if the experimental medication or device is safe and effective. If it is, a new medication or device application is filed with the FDA.
FDA scientists review the study results and determine whether the medication or device is safe and effective enough to be "cleared for marketing." In some cases, an Advisory Committee composed of FDA-appointed experts is convened to review the application and recommend whether it should be approved and, if so, under what conditions. The FDA is not required to accept an Advisory Committee's recommendations, but it typically does accept them.
It took an average of 16.9 months for the FDA to review each medicine it approved in 2003. The proportion of applications rejected at this point in the approval process has remained constant over the years at about 10-15 percent.
Off-Label Use of Drugs & Devices
Once cleared for marketing, the medication or device is available to physicians and patients. In the United States, FDA regulations permit doctors and other health care providers to prescribe approved medications and devices for indications other than the disease or condition for which they are approved; this is called off-label use. Learn more about off-label use here.
Post-marketing, or Phase 4
Patients participating in the clinical trial are followed for a year or more - sometimes many years - after a medication or device receives regulatory approval to monitor for safety and effectiveness and to gather additional information about risks, benefits, and optimal use. Since a much bigger and more diverse group of patients is now likely to take the medicine or have the device, researchers may detect side effects or adverse events that were not apparent during clinical trials. This is why researchers must submit regular reports to the FDA detailing complications they observe. These studies also help researchers better assess how the medication or device affects a particular group of patients based on such criteria as age, sex, race or condition.
Types of Studies
Studies are conducted using varying methods and are commonly classified as observational or interventional. Common study classifications include:
Observational studies meaning that researchers only observe study participants and do not intervene in their care or treatment program. These studies are not considered clinical trials.
Observational retrospective cohort studies collect past data and information from the medical records of two groups of similar human populations who differ in only one key characteristic, to measure a specific outcome. An example of this would be looking for the prevalence of lung cancer in a population of 40-year-old Caucasian women where half of the population smokes tobacco and half do not smoke at all.
Prospective cohort studies follow a similar human population over a certain time period where the population has key differentiating factors with respect to the study. Researchers observe these differentiations to determine how they affect the study's outcome.
Registry studies observe and collect clinical data about the effectiveness and use of a medication or medical device in a human population that has already received the medication or device. These studies are typically broad and do not exclude participants based on age, gender, race, etc.
Case control studies compare a population with a certain medical condition to a very similar population without the medical condition, to determine factors that may lead to the condition.
Interventional studies mean that researchers give study participants a particular medicine or medical device to assess the outcome. Most clinical trials are classified as interventional studies.
First-in-man studies are when a medication or device that has previously been tested on a non-living organism or animal is tested on humans for the first time.
Cost-Effectiveness of Hypertension Treatment by Pharmacists in Black Barbershops(Abstract)
Kelsey B. Bryant, MD, MPH, MS Andrew E. Moran, MD, MPH Dhruv S. Kazi, MD, MSc Yiyi Zhang, PhD Joanne Penko, MS, MPH Natalia Ruiz-Negrón, PharmD Pamela Coxson, PhD Ciantel A. Blyler, PharmD Kathleen Lynch, PharmD Laura P. Cohen, MD, MPP Gabriel S. Tajeu, DrPH, MPH Valy Fontil, MD, MAS Norma B. Moy, BA Joseph E. Ebinger, MD, MS Florian Rader, MD Kirsten Bibbins-Domingo, PhD, MD Brandon K. BellowsPharmD, MS
Originally published15 Apr 2021https://doi.org/10.1161/CIRCULATIONAHA.120.051683Circulation. 2021;143:2384–2394
Background:

In LABBPS (Los Angeles Barbershop Blood Pressure Study), pharmacist-led hypertension care in Los Angeles County Black-owned barbershops significantly improved blood pressure control in non-Hispanic Black men with uncontrolled hypertension at baseline. In this analysis, 10-year health outcomes and health care costs of 1 year of the LABBPS intervention versus control are projected.
Methods:
A discrete event simulation of hypertension care processes projected blood pressure, medication-related adverse events, fatal and nonfatal cardiovascular disease events, and noncardiovascular disease death in LABBPS participants. Program costs, total direct health care costs (2019 US dollars), and quality-adjusted life-years (QALYs) were estimated for the LABBPS intervention and control arms from a health care sector perspective over a 10-year horizon. Future costs and QALYs were discounted 3% annually. High and intermediate cost-effectiveness thresholds were defined as <$50 000 and <$150 000 per QALY gained, respectively.
Results:
At 10 years, the intervention was projected to cost an average of $2356 (95% uncertainty interval, –$264 to $4611) more per participant than the control arm and gain 0.06 (95% uncertainty interval, 0.01–0.10) QALYs. The LABBPS intervention was highly cost-effective, with a mean cost of $42 717 per QALY gained (58% probability of being highly and 96% of being at least intermediately cost-effective). Exclusive use of generic drugs improved the cost-effectiveness to $17 162 per QALY gained. The LABBPS intervention would be only intermediately cost-effective if pharmacists were less likely to intensify antihypertensive medications when systolic blood pressure was ≥150 mm Hg or if pharmacist weekly time driving to barbershops increased.
Conclusions:
Hypertension care delivered by clinical pharmacists in Black barbershops is a highly cost-effective way to improve blood pressure control in Black men.
Immune Mechanisms of Dietary Salt-Induced Hypertension and Kidney Disease(Abstract)
Fernando Elijovich, Thomas R. Kleyman, Cheryl L. Laffer, Annet Kirabo
Originally published7 Jul 2021https://doi.org/10.1161/HYPERTENSIONAHA.121.16495Hypertension. 2021;78:252–260
Salt sensitivity of blood pressure is an independent risk factor for cardiovascular mortality not only in hypertensive but also in normotensive adults. The diagnosis of salt sensitivity of blood pressure is not feasible in the clinic due to lack of a simple diagnostic test, making it difficult to investigate therapeutic strategies. Most research efforts to understand the mechanisms of salt sensitivity of blood pressure have focused on renal regulation of sodium. However, salt retention or plasma volume expansion is not different between salt-sensitive and salt-resistant individuals. In addition, over 70% of extracellular fluid is interstitial and, therefore, not directly controlled by renal salt and water excretion. We discuss in this review how the seminal work by Harry Goldblatt paved the way for our attempts at understanding the mechanisms that underlie immune activation by salt in hypertension. We describe our findings that sodium, entering antigen-presenting cells via an epithelial sodium channel, triggers a PKC (protein kinase C)- and SGK1 (serum/glucocorticoid kinase 1)-stimulated activation of nicotinamide adenine dinucleotide phosphate oxidase, which, in turn, enhances lipid oxidation with generation of highly reactive isolevuglandins. Isolevuglandins adduct to proteins, with the potential to generate degraded peptide neoantigens. Activated antigen-presenting cells increase production of the TH17 polarizing cytokines, IL (interleukin)-6, IL-1β, and IL-23, which leads to differentiation and proliferation of IL-17A producing T cells. Our laboratory and others have shown that this cytokine contributes to hypertension. We also discuss where this sodium activation of antigen-presenting cells may occur in vivo and describe the multiple experiments, with pharmacological antagonists and knockout mice that we used to unravel this sequence of events in rodents. Finally, we describe experiments in mononuclear cells obtained from normotensive or hypertensive volunteers, which confirm that analogous processes of salt-induced immunity take place in humans.
Hypertension research continues being of the utmost importance since hypertension is the worldwide leading cause of mortality and disability, accounting for 10.8 million or 19.2% of all attributable deaths in 2019.1 Also, control rates in the United States had reached 53.8% in 2013 to 2014, but declined to 43.7% in 2017 to 2018, for several reasons.2 Among them, 6% of all patients with hypertension have truly resistant hypertension, and 10% of the latter have the most severe pattern of refractory hypertension.3 Finally, even controlled hypertension is associated with increased residual cardiovascular risk of unclear cause.4
Harry Goldblatt, a forefather of hypertension research, was stimulated by observations as a clinician (lack of hypertension in a patient dying of uremia after accidental removal of a horseshoe kidney) and as a pathologist (presence of renal arteriolar abnormalities in the autopsies of hypertensive patients) to hypothesize that hypertension required the presence of the kidneys. To explore the controversy on whether the renal arteriolar abnormalities were the cause or consequence of hypertension, he decided to mimic the situation of renal ischemia by constricting the main renal arteries of dogs. He was very cognizant of the difference between such a model and the intrarenal vascular abnormalities of essential hypertension but proceeded with it nonetheless as the most feasible method to reproduce the suspected mechanism of renal ischemia.5
The revolutionary consequences of the results of his experiments were 2-fold. First, the recognition that renal artery stenosis was sufficient to produce sustained blood pressure (BP) elevation, later leading to the recognition of renovascular hypertension in humans. Most importantly, after preliminary investigations on possible mechanisms, Goldblatt postulated that one or more humoral factors produced by the kidneys needed to be involved. A few years later, Page and Braun Menendez simultaneously identified Ang II (angiotensin II)6,7 which began a century of additional research on the role of this peptide in BP regulation.
Gavras et al8 showed that dependency of BP on the renin-angiotensin system in rat models of Goldblatt hypertension was linked to the status of salt balance (natriuresis by the unclipped kidney with persistent hyperreninemia in the unilateral model [2K-1C], as opposed to sodium [Na+] retention and renin suppression in the bilateral one, 1K-1C).9 The group of Laragh at Cornell proposed that Goldblatt’s findings were, therefore, applicable to essential hypertension because the heterogeneous arteriolar lesions of this disorder resulted in some ischemic glomeruli with impaired Na+ excretion, and other nonischemic, hyperfiltering ones with enhanced natriuresis.10
The interplay between Ang II and salt in BP regulation acquired a new dimension once it was demonstrated that tissue-generated Ang II played ubiquitous roles in growth, proliferation and organ damage, central nervous system regulation of sympathetic tone, and most importantly, in renal Na+ transport by direct actions on transporters and by stimulation of aldosterone release.
More recently, a series of seemingly unrelated observations suggested participation of immunity and inflammation in the pathogenesis of hypertension. For example, hypertension was produced in normal rats by transfer of lymphocytes from rats with renal infarction or from splenocytes of rats with deoxycorticosterone acetate-salt hypertension.11,12 Conversely, immunosuppressants, thymectomy, antithymocyte serum, or transplant of a normal thymus prevented or reversed hypertension in several hypertensive rodent models.11,13–15 A direct link between these observations and the previously recognized interplay between Ang II and Na+ was provided by Guzik et al,16 who showed that Ang II and deoxycorticosterone acetate-salt hypertension were attenuated in mice genetically lacking lymphocytes.
Other investigators showed that Na+ is involved in immune disorders unrelated to hypertension, for example, experimental encephalomyelitis.17 We embarked on the investigation of how Na+ may trigger immune changes that underlie the pathophysiology of hypertension.
Dual Antiplatelet Therapy After Percutaneous Coronary Intervention and Drug-Eluting StentsA Systematic Review and Network Meta-Analysis(Abstract)
Safi U. Khan, MD Maninder Singh, MBBS Shahul Valavoor, MD Muhammad U. Khan, MD Ahmad N. Lone, MD Muhammad Zia Khan, MD Muhammad Shahzeb Khan, MD Preethi Mani, MD Samir R. Kapadia, MD Erin D. Michos, MD, MHS Gregg W. Stone, MD Ankur Kalra, MD Deepak L. BhattMD, MPH
Background:
The optimal duration of dual antiplatelet therapy (DAPT) after percutaneous coronary intervention with drug-eluting stents remains uncertain. We compared short-term (<6-month) DAPT followed by aspirin or P2Y12 inhibitor monotherapy; midterm (6-month) DAPT; 12-month DAPT; and extended-term (>12-month) DAPT after percutaneous coronary intervention with drug-eluting stents.
Methods:
Twenty-four randomized, controlled trials were selected using Medline, Embase, Cochrane library, and online databases through September 2019. The coprimary end points were myocardial infarction and major bleeding, which constituted the net clinical benefit. A frequentist network meta-analysis was conducted with a random-effects model.
Results:
In 79 073 patients, at a median follow-up of 18 months, extended-term DAPT was associated with a reduced risk of myocardial infarction in comparison with 12-month DAPT (absolute risk difference, –3.8 incident cases per 1000 person-years; relative risk, 0.68 [95% CI, 0.54–0.87]), midterm DAPT (absolute risk difference, –4.6 incident cases per 1000 person-years; relative risk, 0.61 [0.45–0.83]), and short-term DAPT followed by aspirin monotherapy (absolute risk difference, –6.1 incident cases per 1000 person-years; relative risk, 0.55 [0.37–0.83]), or P2Y12 inhibitor monotherapy (absolute risk difference, –3.7 incident cases per 1000 person-years; relative risk, 0.69 [0.51–0.95]). Conversely, extended-term DAPT was associated with a higher risk of major bleeding than all other DAPT groups. In comparison with 12-month DAPT, no significant differences in the risks of ischemic end points or major bleeding were observed with midterm or short-term DAPT followed by aspirin monotherapy, with the exception that short-term DAPT followed by P2Y12 inhibitor monotherapy was associated with a reduced risk of major bleeding. There were no significant differences with respect to mortality between the different DAPT strategies. In acute coronary syndrome, extended-term in comparison with 12-month DAPT was associated with a reduced risk of myocardial infarction without a significant increase in the risk of major bleeding.
Conclusions:
The present network meta-analysis suggests that, in comparison with 12-month DAPT, short-term DAPT followed by P2Y12 inhibitor monotherapy reduces major bleeding after percutaneous coronary intervention with drug-eluting stents, whereas extended-term DAPT reduces myocardial infarction at the expense of more bleeding events.
Mapping overdiagnosis of thyroid cancer in China
Globally, the incidence of thyroid cancer has increased substantially in the past three decades,particularly among young adults and even in adolescents,whereas mortality due to thyroid cancer has remained relatively stable at low levels, or decreased, almost everywhere.The intense scrutiny of the thyroid gland and widespread use of ultra- sonography and other modern diagnostic techniques have allowed the discovery of a large reservoir of previously undetectable, small, and predominantly papillary thyroid tumours. Thus, the epidemic of thyroid cancer is likely to be predominantly driven by overdiagnosis—ie, the diagnosis of cancer that would not go on to cause symptoms or death in a patient’s lifetime. Overdiagnosis of thyroid cancer has been estimated to account for up to 60–90% of the diagnosed cases in several countries.
This phenomenon might be affecting China,1 where thyroid cancer is the fastest growing cancer, with an average 20% annual increase over 2003–11.However, substantial geographical variability exists, with an approximately 45 times difference between areas with lowest and highest incidence,5 the reasons for which remain unclear.
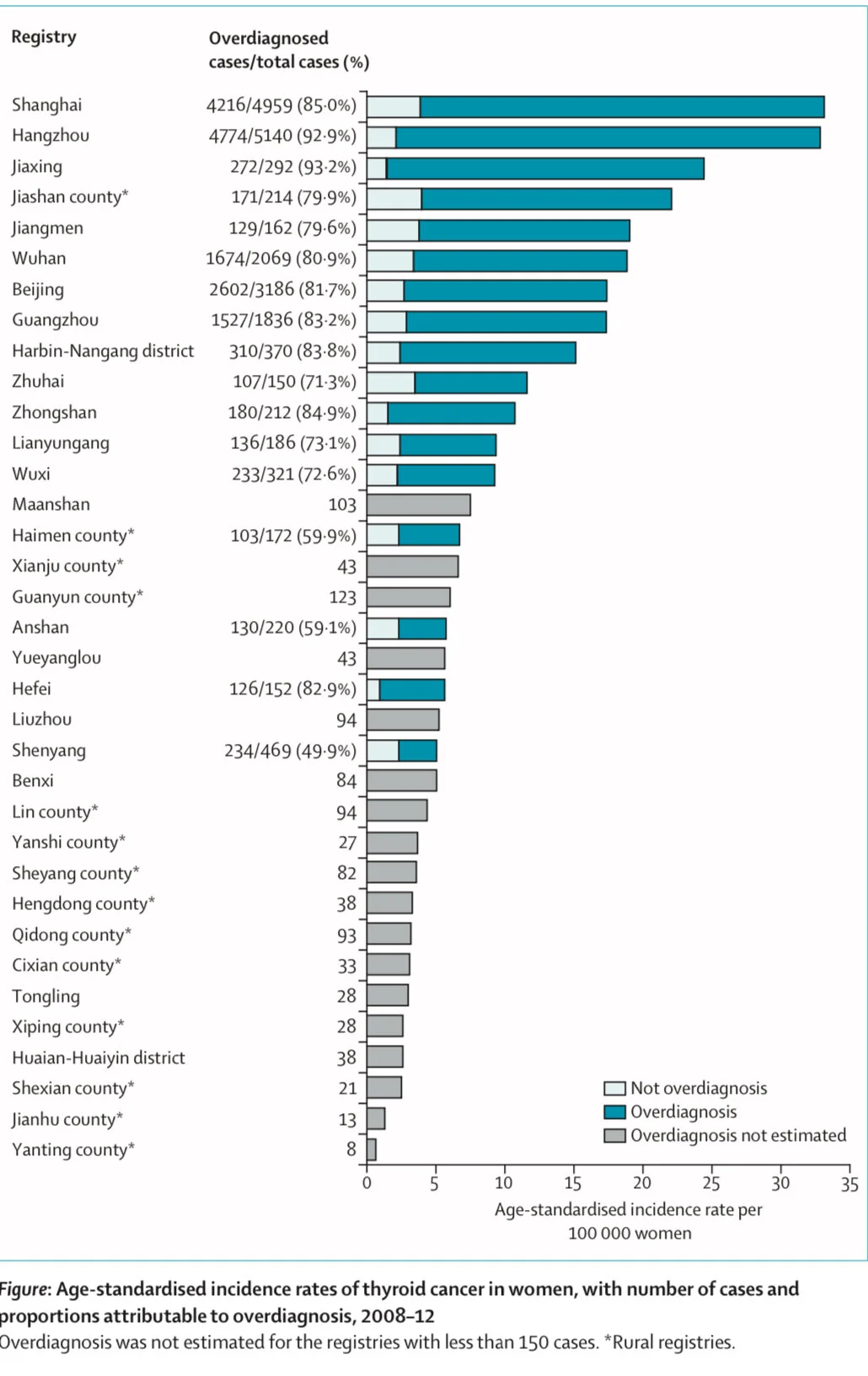
In this study, we explored the epidemiological features and the impact of overdiagnosis on thyroid cancer across regions of China, using population-based data from 35 cancer registries in mainland China included in the Cancer Incidence in Five Continents (CI5) database for the period 2008–12. In this period, 27 842 individuals aged 15–84 years were diagnosed with thyroid cancer (appendix pp 2–5). The average age- standardised incidence rate was 16.8 cases per 100000 women and 5·3 cases per 100 000 men. We found a large variability across registries in the age-standardised incidence of thyroid cancer, ranging from 0.7 to 33.9 cases per 100 000 women (figure) and from 0·4 to 11.6 cases per 100 000 men (appendix p 6). Higher incidence rates were observed in the 21 urban registries (an average age- standardised incidence 19.0 cases per 100000 women and 6·1 cases per 100000 men) than in their rural counterparts (4·9 cases per 100000 women and 1.4 cases per 100000 men). This geographical variation reflected predominantly the incidence of papillary carcinoma, which accounted for most of the diagnosed thyroid cancer cases in all registries (appendix p 7).
For ten registries with at least 10 years of registration data available (for 2003–12), we also assessed the temporal change of age-standardised incidence rates from 2003–07 to 2008–12, in absolute terms and as percentage of variation. We found increases of more than 10 cases per 100000 women and 5 cases per 100 000 men, with relative changes during this period exceeding 100% in Shanghai, Jiaxing, and Jiashan county (appendix p 12).
Contrary to incidence and similarly to what has been observed in other countries,thyroid cancer mortality remains low in China Previous studies have shown that the age-standardised mortality rate of thyroid cancer was 0·35 deaths per 100 000 women and 0.19 deaths per 100 000 men in 2010,far below the observed incidence, with an incidence-to-mortality ratio exceeding 40 in women and 20 in men. Even in high-incidence areas such as Zhejiang province, where the registries of Hangzhou, Jiaxing, and Jianshan county are located, age- standardised mortality of thyroid cancer remained stable at relatively low levels in the period 2000–12.7
A distinct epidemiological feature of thyroid cancer overdiagnosis that has been observed globally is that the increase in incidence is typically accompanied by a shift of the age at diagnosis, with a peak at around middle age (35–64 years), instead of at older ages (65–84 years), as was observed before the 1980s.Indeed, when plotting incidence against age at diagnosis in 2008–12 many regions of China followed this pattern, resembling an inverted U-shape, which was particularly pronounced in urban areas with high age-standardised incidence rates and large cities like Shanghai and Hangzhou (appendix p 8) but much less prominent in rural registries, except for Jiashan county (appendix p 9). Women in particular were found to be diagnosed early in life (age 30–49 years), probably due to their greater access to the health system than men due to gynaecological and obstetrical reasons, leading to increased chance of having their thyroid scrutinised by ultrasound. Unfortunately, data on the number of ultrasound machines in the study areas are not available.
We calculated overdiagnosis on the basis of the difference between the observed and the expected age-specific incidence, where the expected age curve was assumed to correspond to a scenario without overdiagnosis (ie, incidence increasing with a power law of age, as in historical patterns and in agreement with the multistage model of carcinogenesis; appendix pp 2–3). For all 21 registries in urban areas combined, we estimated that overdiagnosis accounted for 16 721 (83.1%) of 20 114 thyroid cancer cases in women and 4986 (77.3%) of 6452 cases in men in 2008–12. The highest proportions of overdiagnosis were estimated for Shanghai, Hangzhou, Wuhan, Beijing, and Guangzhou, accounting for over 70% of all thyroid cancer cases for both sexes (figure; appendix p 6). For all 14 rural registries combined, we estimated that 597 (60.4%) of 989 thyroid cancer cases among women and 170 (59.2%) of 287 cases among men were overdiagnosed.
We further assessed the possible role of availability and access to health care in China that, together with screening prevalence and socioeconomic development, has been found to be positively associated with incidence of thyroid cancer in previous national and international studies.We found that the age-standardised incidence of thyroid cancer was strongly associated at the regional level with gross domestic product (GDP) per capita and with the number of hospital beds per 1000 people in both sexes (appendix pp 10). One unit (¥10 000) increase in log(GDP) was associated with a 0.93 (95% CI 0.51–1.36) times increase of log(age-standardised incidence) in women and a 0.90 (0.50–1.31) times increase of log (age-standardised incidence) in men. The corresponding Spearman correlation coefficient was 0.52 (p=0.0017) in women and 0.60 (p=0.0002) in men. The regression coefficient of log(age-standardised incidence) on log-transformed number of hospital beds per 1000 people was 0.83 (95% CI 0.38–1.28) in women and 0.83 (0·42–1·24) in men; and the corresponding Spearman correlation coefficient was 0.44 (p=0.010) in women and 0.52 (p=0·0019) in men. Similar findings were observed when we only included the papillary thyroid cancer cases (appendix p 11).
Despite limitations due to possible ecological fallacy, we found that overdiagnosis of thyroid cancer occurs more often in regions where people have increased accessibility and affordability of health care than in other areas. No organised screening programmes for thyroid cancer exist in China, but the unregulated nature of the offer of medical services might lead to a large number of unnecessary check-ups. Thyroid ultrasound is included in the checklist of services in many health examination centres in China, especially under the scheme of urban employee-based basic medical insurance. The predominant fee-for- service payment method might have worsened the situation by creating incentives for hospitals to encourage more examinations. A national survey showed that the prevalence of thyroid nodules detected by ultrasonography was 20·4% in adults from the general populations.The large reservoir of subclinical disease in the general population, combined with the increasing use of non-evidence-based and extensive examinations, might have driven the high proportion of overdiagnosis in the urban areas.
Although rural areas were less affected by overdiagnosis than their urban counterparts, overdiagnosis cannot be ignored in these areas for at least two reasons. First, uneven development was seen within rural areas. For example, Jiashan county, where we observed substantial overdiagnosis, is among the top 100 counties in China in terms of comprehensive strength and development. Second, the rate of urbanisation has been accelerating in China over the past four decades. With the fast socioeconomic transition, the trends of thyroid cancer overdiagnosis observed in urban areas could potentially spread to rural areas if no regulation measures are available.
In conclusion, we found that many registries in China, predominantly in urban areas, seem to display the typical epidemiological features of overdiagnosis of thyroid cancer. These features include a large geographical variability in the incidence of the disease; a fast increase in incidence over a short period of time without a corresponding increase in mortality; a large proportion of papillary carcinomas; a great distortion of age-specific curves; and a positive correlation with indicators that are proxies of availability and access to health care, such as GDP per capita and number of hospital beds, suggesting that overdiagnosis has a major role in the regional variation of incidence of thyroid cancer.
Overall, our analyses indicate a possible sizeable problem of over- diagnosis of thyroid cancer in several urban cities in China. Individuals who are overdiagnosed with thyroid cancer undergo heavy and unnecessary treatments (including surgical removal of the thyroid gland and lifelong hormonal replacement therapy), which implies substantial impairment of patients’ quality of life and also relevant economic costs for patients and the health system. Thyroid cancer overdiagnosis is an example of medical service overuse, which is a major challenge to increase health service equality and reduce the governmental expenditure simultaneously. Our findings from China—a country rapidly transitioning to a higher level of socioeconomic status—should be an early warning to this emerging economy and other countries at a similar stage of development.